Alzheimer’s disease (AD) is the most common cause of dementia, yet scalable early screening remains challenging. Current risk assessment relies heavily on neuroimaging (e.g., Aβ/tau PET, FDG-PET, structural MRI), which is expensive, less accessible, and difficult to deploy for population-level longitudinal surveillance. This project explores a low-threshold alternative: using intestinal disease phenotypes as early, trackable markers of long-horizon AD risk, grounded in the gut–brain axis.
Growing evidence suggests that gastrointestinal disorders (through microbial dysbiosis, immune activation, altered intestinal and blood–brain barrier permeability, and metabolite-mediated neuroimmune signaling) may act as upstream triggers or amplifiers of neurodegeneration. Importantly, many intestinal diseases occur years to decades earlier than typical AD onset, offering valuable lead time for prevention-oriented risk stratification.
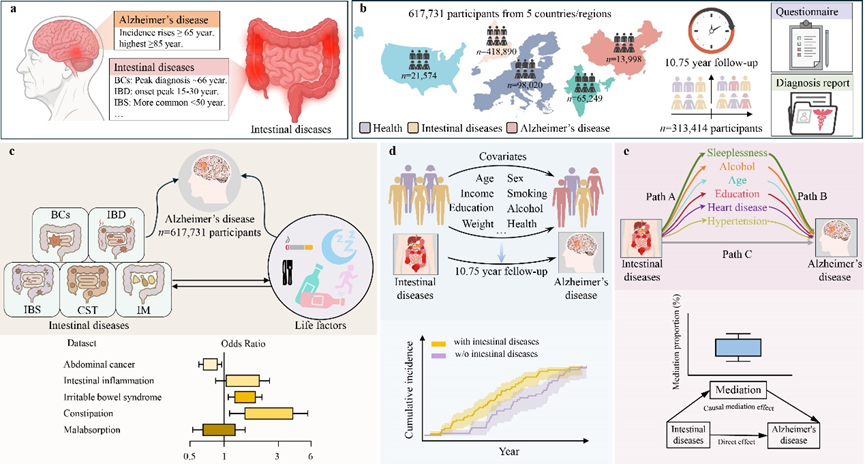
We conducted a large-scale, multi-country prospective cohort study across Asia, Europe, and the Americas, comprising 617,731 participants (including 313,414 participants from four countries with an average follow-up of 10.75 years). Using harmonized diagnostic records (e.g., UK Biobank and other nationally representative cohorts), we investigated five common gastrointestinal conditions: bowel cancers (BCs), inflammatory bowel disease (IBD), irritable bowel syndrome (IBS), constipation (CST), intestinal malabsorption (IM).
We quantified their associations with incident AD using time-to-event models, evaluated heterogeneity via systematic effect-modifier analyses, and strengthened directional inference by performing causal mediation analysis to estimate indirect effects through modifiable behaviors, with robustness checks via nonparametric bootstrap and sensitivity analyses.
This work establishes a disease-anchored gut–brain biomarker strategy for early AD risk stratification—reusable, trackable, and scalable using routinely collected clinical records. By shifting part of risk assessment from resource-intensive neuroimaging to accessible gastrointestinal phenotypes (and their behavioral mediators), the project provides a pragmatic framework for population-level prevention, targeted follow-up, and earlier intervention planning.